Estimates of the number of births and deaths in India every year come from two key sources: the Civil Registration System (CRS) which relies on registered events, and the Sample Registration System (SRS), which is a large demographic survey. In this article, we look at how the two systems evolved, their methodologies, uses, and the key debates around them.
Evolution of birth and death estimation in India
The Civil Registration System (CRS)
The history of civil registration in India dates back to the mid-19th century. Before independence, birth and death registration existed in certain provinces, but enforcement was weak and lacked uniformity.
After independence, the Indian government needed standardised demographic data to support the country's five-year development plans leading to the establishment of the Office of the Registrar General, India (RGI) in 1951.[1] In 1958, the RGI published its first annual report using civil registration data, making it the first precursor of what would become the CRS's annual report. The Registration of Births and Deaths (RBD) Act, 1969, made birth and death registration mandatory across India and provided a legal framework for uniform nationwide implementation of civil registration.
Despite its legal mandate, under-registration and irregular reporting problems persisted, making the analysis of trends from CRS-based data almost impossible.
In 2000, the system was revamped to enhance data quality and streamline reporting. The 2023 CRS report showed significant progress, with 98.4% of births and 97.2% of deaths registered.[2] The Registration of Births and Deaths (Amendment) Act, 2023, made the birth certificate the sole official document for proof of date and place of birth. The amendment also mandated the digitisation of CRS records and integration with national databases such as Aadhaar, electoral rolls, and the population register.
The Sample Registration System (SRS)
The SRS was introduced in the 1960s as an interim measure to provide reliable estimates of birth and death rates at a time when CRS was incomplete and lacked nationwide coverage. At first, the RGI initiated the SRS, a sample based vital registration system, as a pilot project in 1964-65 in selected states. Encouraged by the success of the pilot, the system was expanded to full-scale operations in 1969-70.
Over the years, SRS expanded in both scope and methodology. By 2023, the sample had grown to 8,839 units, covering more than 8.8 million people, making it one of the largest demographic surveys worldwide.
Over time, SRS data collection gradually expanded beyond fertility and mortality indicators. Birth interval and birth order statistics were added in 1990, population distribution by marital status in 1992, and fertility rates by education level in 1996.[3] The first maternal mortality estimates (1997-2003) were published in 2006, followed by the first cause of death report (2001-03) in 2009. Since then, maternal mortality bulletins and cause of death statistics have been published periodically.
The baseline survey was expanded in 2004 to include household conditions, morbidity, personal habits such as tobacco and alcohol use, and reproductive health indicators.[4] In 2014, the system was fully digitised, and by 2021, handheld data collection devices were replaced with mobile applications to enhance efficiency.
The last available data from the sample registration system was released for the year 2023 in 2025. The last sample replacement was in 2015, and the next sample replacement was expected in 2024, following the decadal census of 2021. However, the next census is now scheduled in 2027, and the subsequent SRS sample replacement is expected to follow thereafter.
Methodologies
How the CRS functions
The CRS aims to record all births, deaths, and stillbirths in a continuous, permanent, and compulsory manner under the Registration of Births and Deaths Act. Unlike the Sample Registration System, which estimates vital rates based on a sample, the CRS aims to capture every birth and death occurring in the country.
The Office of RGI oversees the CRS and coordinates with Chief Registrars of Births and Deaths in each state and union territory. Once a birth or death occurs, an informant must report it to the local registrar within 21 days. Birth/Death can be registered at the place of occurrence only.
After registration, the registrar issues a birth or death certificate. If an informant reports a birth or death after 21 days, penalties range from a late fee to an order from the Executive Magistrate depending on the length of the delay. CRS annually publishes reports that provide state-level and district-level data on registered births, deaths, infant deaths, and stillbirths across India usually with a time lag of two years. The reports include detailed statistical tables, charts, and analysis on registration completeness, sex-wise distribution, medical attention at birth and death, and the timeliness of birth and death registration. The raw data is not publicly available.
How the SRS is conducted
Selecting the sample
The SRS aims to provide reliable estimates of key demographic indicators at the natural division[5] and state levels for major states[6], at the state level for smaller states, and at the national level.
It follows a single-stage, stratified simple random sampling design, except in larger villages where two-stage stratification is used. The sampling frame consists of villages or village segments in rural areas and census enumeration blocks in urban areas, from which a set of units is randomly selected. These frames and units are updated after each census.
The number of villages and urban blocks are determined by the population that would be needed to accurately estimate the infant mortality rate with an acceptable margin of error[7], along with financial and operational constraints. In 1970, the SRS covered over 3,600 villages and urban blocks. The sample size increased significantly in 1982, covering more than 6,000 sampling units. By 2023, the SRS had expanded further, including over 8,800 villages and urban blocks and covering a population of more than 8.8 million.
Once the villages and urban blocks are selected, SRS covers all households in these units through a combination of continuous enumeration and biannual independent surveys. It records vital events in the same units for the next ten years or until the next census sampling frame becomes available.
Conducting the survey
Once the sample is updated, a new baseline survey is conducted before data collection, recording household members' demographic details. Following this, a part-time enumerator, usually a local anganwadi worker or teacher residing in the sample unit, continuously records all births and deaths within their sampling unit, as well as those of usual residents occurring outside it. They gather information from families, community informants such as the village priest, barber, village head or midwife, as well as from hospitals and burial or cremation grounds to maximise event recording. To minimise missing data, they visit all households once a month in urban areas and once every three months in rural areas to verify and update records.
Every six months, a full-time supervisor visits each household in the sample unit and conducts an independent retrospective survey to record past vital events. Supervisors also fill out the Verbal Autopsy questionnaires for each death identified during the half-yearly survey.[8]
After the half-yearly survey, the Directorate of Census Operations office matches the supervisor's records with the enumerator's to identify omissions, errors, or duplications. To verify unmatched or partially matched events, a third person or a team consisting of the supervisor and enumerator visits the households, depending on staff availability.
The sampling unit supervisor updates the population of each sample unit by age, sex, and marital status and records the results of the matching and verification exercises. The supervisor then submits this information, along with updates to household numbers and schedules, to the RGI office in Delhi for national tabulation, analysis, and publication.
Data dissemination
The RGI regularly publishes data from the SRS. The annual bulletin reports crude birth and death rates along with the infant mortality rate for India and its states. The annual statistical report, published with an average time lag of two years, provides detailed estimates of population composition, fertility and mortality rates, and medical attention received at birth or death by state and selected demographic characteristics such as place of residence (urban and rural), age, and sex.
Reports on maternal mortality and causes of death are published less frequently, as multiple years of data are required to ensure a sufficient number of cases for state- and age-sex-specific analysis. Life tables, which provide sex- and age-specific death patterns and life expectancy, are published using data aggregated over five years. These tables are further disaggregated by location (urban and rural) for each state and the country as a whole.
Unlike the National Sample Survey (NSS) and the National Family Health Survey (NFHS), the SRS does not release the unit-level data.
Uses of SRS and CRS data
SRS data is widely used by researchers to study India's population dynamics and demographic transitions at both the national and state levels.
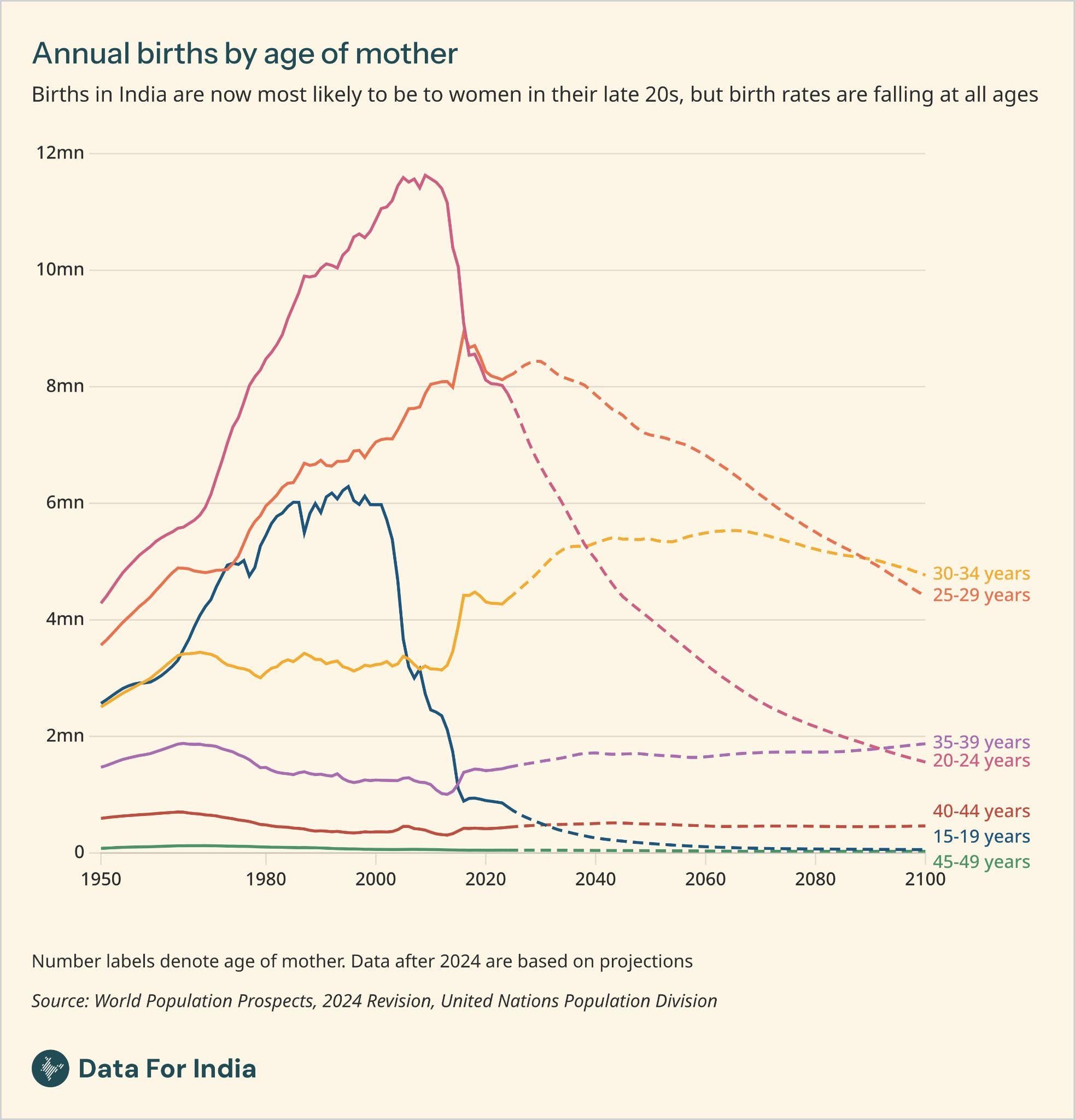
The UN Population Division and the Registrar General of India heavily rely on SRS estimates to produce population projections. These projections play a crucial role in informing healthcare planning, education policies, infrastructure development, economic strategies, and environmental sustainability. Additionally, SRS records have been used for census evaluation studies. Studies have leveraged SRS data to analyse birth and death trends, track India's demographic transition[9], and assess changes in population growth, age structure, and sex composition.[10]
Researchers have used SRS data to analyse the pace of fertility decline, showing that while many states have approached or surpassed replacement fertility, regional disparities persist.[11]
SRS data has also been instrumental in studying disparities in child mortality across India.[12] Researchers have used SRS data to analyse gender differences in life expectancy across India and states, highlighting a shift from male longevity in the 1970s to a female advantage by the 2000s.[13]
Researchers have extensively utilised SRS data to examine trends, patterns, and sub-national disparities in maternal mortality across India over the past two decades.[14] Moreover, SRS estimates of MMR play a key role in tracking the effectiveness of maternal health programmes enabling policymakers to assess progress, identify high-risk regions, and refine intervention strategies to improve maternal health outcomes across India. Policymakers have also used SRS data to set demographic and health targets in national population policies.
While the CRS has historically faced challenges such as incomplete coverage and delays in data reporting, recent improvements in registration completeness and more timely publication of data have allowed researchers to use CRS data to analyse mortality patterns highlighting its growing relevance for demographic analysis in India.[15]
Issues with the CRS and SRS
Under-registration of deaths in the CRS has been a persistent issue across many states. The level of suggested under-reporting in death registration by the CRS varies substantially from state to state, with only a third of deaths as estimated from the SRS registered in Nagaland for instance, in 2023. Among the major states Bihar reported the lowest level of death registration with every other death not registered with CRS. The level of under-reporting is also higher in rural areas and among women.
A primary study in Bihar found that, other than the lack of awareness, most participants did not report child or adult female deaths due to the absence of financial or property-related benefits. They faced challenges in birth and death registration due to poor service delivery, high indirect costs, and bribe demands by CRS staff. The study also highlighted insufficient investment, staff shortages, and inadequate digital infrastructure at registration centers.[16]
Moreover, the number of births and deaths registered in the CRS show large fluctuations in some states over the years. For instance, in Assam, the number of registered births rose from over 723,000 in 2014 to over a million in 2015, before returning again to over 734,000 in 2016, reflecting fluctuations that suggest possible inconsistencies in registration coverage or data reporting. Similarly, for Madhya Pradesh, registered deaths dipped from over 372,000 in 2013 to under 311,000 in 2015, but then rose again to over 370,000 in 2017.
Researchers have also repeatedly highlighted inconsistencies and unrealistic patterns in the computation and reporting of child mortality data in SRS.
One such major inconsistency observed was the apparent stagnation and reversal in child mortality trends during 1995 to 2005. Despite improvements in healthcare and overall life expectancy, child mortality, especially among girls, showed an increasing trend in several states in the mid 1990s and early 2000s-an unexpected pattern in demographic analysis. The ratio of child mortality to infant mortality in official life tables appeared unrealistically high, defying empirical trends observed globally. A reassessment of SRS life tables suggested that child mortality was likely overestimated, while female life expectancy was likely underestimated.[17]
Another major issue highlighted is internal discrepancies within SRS reports on early childhood mortality in recent years. A comparison of age-specific death rates (ASDR) and infant mortality rates (IMR) from the 2018 SRS Statistical Report[18] found inconsistencies in several states.[19]
Given challenges with both systems, there is a debate over which dataset is more reliable and provides better estimates. The SRS remains the stable source of national and state-level demographic estimates in India, supporting the regular tracking of births and deaths, population projections, and assessments of registration completeness under the CRS. States with better administrative capacity have moved closer to universal registration through the CRS, allowing for the use of the CRS to track birth and deaths in these states. However, improvements in the CRS have been uneven across the country, with several states still recording low levels of registration. As a result, the SRS is likely to remain central for producing reliable and comparable vital statistics in states where civil registration continues to lag.
[1] Both CRS and SRS operate under the Registrar General of India (RGI), Ministry of Home Affairs, the same body that conducts the decadal census.
[2] The CRS uses the SRS birth and death rates and multiplies them by the projected mid-year population of the corresponding year to derive the estimated number of births and deaths for India and states. The number of CRS registered births and deaths are then divided by the estimated number of births and deaths to calculate the proportion of births and deaths registered in the CRS.
[3] The Sample Registration System (SRS) in India, An Overview (2017), Prasanta Mahapatra.
[4] This data, however, is not publicly available.
[5] Natural regions are sub-state study domains used in the National Sample Surveys. These regions are formed by grouping contiguous districts based on geographical features and population densities.
[6] States with a population of ten million or more as per the 2011 Census.
[7] The computation of sample size requires an input estimate of a key indicator, taken from previous surveys, to be plugged into a statistical formula. In the case of SRS, this indicator is the Infant Mortality Rate (IMR), which measures how many babies die before their first birthday per 1,000 live births. The sample size is determined in such a way that IMR can be estimated with good accuracy. Specifically, the aim is to keep the Relative Standard Error (RSE) below 15%. RSE tells us how precise the estimate is-a lower RSE means the estimate is more reliable. In larger states, this level of precision is targeted at the level of natural regions, while in smaller states and union territories, it is ensured at the overall state level.
[8] The supervisor conducts a Verbal Autopsy (VA) interview using a questionnaire called the 'Routine, Representative, Resampled, Household Interview of Mortality with Medical Evaluation' (RHIME) method. This method collects information about the circumstances and symptoms leading to a person's death. The questionnaire varies based on the age and sex of the deceased, with specific forms for infants, children, adults, and maternal deaths. After completing the interview, two trained physicians independently review the information and determine the Cause of Death (COD) using the International Classification of Diseases, 10th Revision (ICD-10), which standardises codes for different diseases and health conditions. If the physicians disagree, they discuss the case to reach a consensus, and if needed, a third physician makes the final decision. To ensure accuracy, supervisors randomly select 10% of the VAs for rechecking. During this process, another supervisor conducts a fresh interview to verify the findings. Two separate physicians also review and assign a COD for these quality-check VAs.
[9] Demographic Changes in India: Is the Country Prepared for the Challenge? (2016), KS James and S Goli, The Brown Journal of World Affairs.
[10] Demographic Transition in India: Insights Into Population Growth, Composition, and Its Major Drivers (2021), Usha Ram and Faujdar Ram, Oxford Research Encyclopedia of Global Public Health.
[11] India's Changing Dates with Replacement Fertility: A Review of Recent Fertility Trends and Future Prospects, P.N. Mari Bhat.
[12] Trends in geographical mortality differentials in India (2010), Nandita Saikia et al., MPIDR Working Paper.
[13] Gender Gap in Life Expectancy in India (1970-2006), Vladimir Canudas-Romo and Nandita Saikia, IEG Working Paper.
[14] Maternal Mortality in India: A Review of Trends and Patterns (2015), William Joe et al., IEG Working Paper.
[15] Assessing mortality registration in Kerala: the MARANAM study (2022), Aashish Gupta & Sneha Sarah Mani, Genus-Journal of Population Sciences
[16] Performance barriers of Civil Registration System in Bihar: An exploratory study (2022), Krishna Kumar et al., PLOS One.
[17] Has Child Mortality in India Really Increased in the Last Two Decades? (2010), Nandita Saikia et al., Economic and Political Weekly.
[18] IMR is computed as 1000 × (number of infant deaths during the year / number of live births during the year), while ASDR for age 0-1 is computed as 1000 × (number of deaths in the age group 0-1 during the year / midyear population in the age group). While the numerator in the computation of IMR and ASDR is the same, the denominator differs. In a given year, the midyear population of age 0-1 must be lower than the total births in the same year, as some newborns may not survive their first year. This should result in IMR always being lower than ASDR (0-1). Theoretically, IMR should never exceed ASDR (0-1) under any condition. Additionally, if the ratio of ASDR to IMR exceeds five percentage points, it indicates a potential issue with the denominator used in computing these rates.
Ideally, the ASDR-to-IMR ratio should remain within a narrow range (within 5%), but states like Uttar Pradesh (59%), Gujarat (48%), and Rajasthan (35%) reported significantly higher discrepancies.
[19] The SRS Data on Early Childhood Mortality in India (2021), Usha Ram et al., Economic and Political Weekly.